In perioperative medicine, the route of drug administration profoundly affects the speed, reliability, and comfort of medication delivery. Transmucosal administration — using mucous membranes as the entry point — offers a compelling alternative to both intravenous and oral routes, particularly in contexts where speed matters and needle access is undesirable.
How Transmucosal Delivery Works
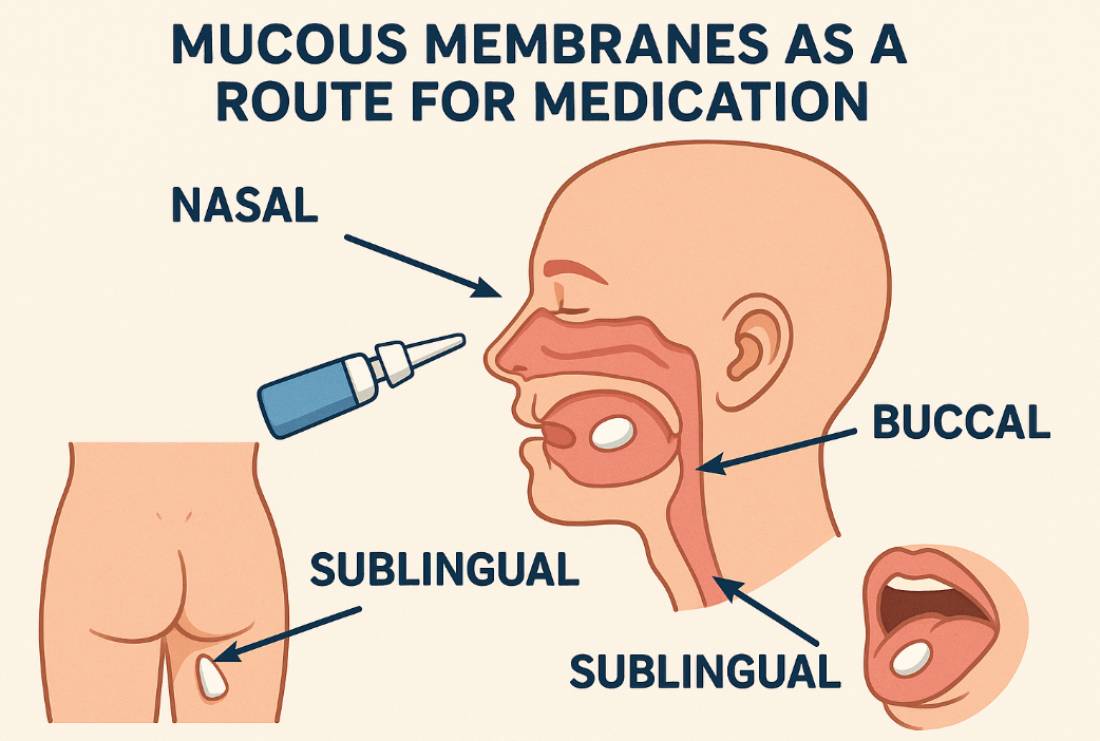
Mucous membranes line various body cavities including the nasal passages, oral cavity, sublingual tissues, and rectum. These surfaces are richly vascularized and permit rapid absorption of appropriately formulated medications directly into the bloodstream — bypassing the gastrointestinal tract and avoiding first-pass hepatic metabolism.
This bypass is clinically significant. Oral medications must survive gastric degradation and hepatic processing, which reduces bioavailability and slows onset. Transmucosal medications enter the systemic circulation more directly, providing onset times that can approach those of intravenous administration.
Key Advantages
- Rapid onset: Absorption through highly vascularized mucosal surfaces can produce effects within minutes
- No needle required: Eliminates needle-related pain and anxiety — particularly valuable for pediatric patients and needle-phobic adults
- Enhanced bioavailability: First-pass metabolism is reduced or eliminated, allowing more drug to reach systemic circulation
- Non-invasive: Can be administered by patients, caregivers, or clinical staff without specialized equipment
Clinical Applications in Anesthesia and Analgesia
Intranasal Fentanyl
Among the most studied transmucosal analgesics in perioperative and emergency care, intranasal fentanyl demonstrates efficacy comparable to intravenous opioids in multiple clinical settings. Clinical trials show it achieves superior pain reduction within the first 15–20 minutes in children with acute injuries.
A key advantage is the avoidance of intravenous access — in pediatric patients especially, the distress of IV placement can exceed the distress of the painful condition itself. Intranasal fentanyl via atomizer devices delivers predictable, titratable analgesia without this barrier.
Sublingual and Buccal Medications
Sublingual (under the tongue) and buccal (inner cheek) routes are used for a variety of anesthesia-related medications including sublingual midazolam for procedural anxiolysis in children, buccal lorazepam for seizure management, and buprenorphine for pain management applications.
Intranasal Dexmedetomidine
Intranasal dexmedetomidine has emerged as an effective premedication for pediatric patients undergoing anesthesia, providing sedation and anxiolysis without respiratory depression — making it particularly useful for mask induction or procedural sedation preparation.
Challenges and Limitations
Transmucosal administration is not without constraints that limit its universal applicability:
- Limited volume capacity: Mucosal surfaces can only absorb small volumes; high-dose medications requiring large volumes are not suitable for this route
- Variability in absorption: Mucus layers, nasal congestion, saliva flow, and anatomical variations all affect drug uptake — introducing pharmacokinetic unpredictability
- Drug-specific requirements: Not all medications are suitable; drugs must be potent enough at low volumes, appropriately formulated (correct pH, particle size), and lipophilic enough for mucosal penetration
- Formulation complexity: Specialized delivery systems (atomizers, nasal sprays, films) are required for reliable, consistent delivery
An Advancing Frontier
Transmucosal drug delivery represents a growing area of pharmacological innovation. As formulation science advances and more agents are validated for mucosal routes, this approach will expand beyond its current applications in pain management and pediatric sedation. For anesthesia providers, understanding its pharmacokinetics — and its limitations — is essential to safe, effective use.